
Accupril
"Buy generic accupril 10 mg line, medications voltaren".
By: K. Kliff, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Deputy Director, Universidad Central del Caribe School of Medicine
Cheap 10mg accupril with mastercard
The anterior and posterior fontanels are tense even when the patient is in the upright place medicine information purchase accupril 10 mg line. With continued enlargement of the mind medical treatment 80ddb order accupril with amex, torpor units in and the toddler appears languid medications known to cause weight gain generic accupril 10mg free shipping, bored with his surroundings medicine 5325 purchase cheap accupril online, and unable to sustain exercise. This is the "setting-sun sign" and has been incorrectly attributed to downward pressure of the frontal lobes on the roofs of the orbits. The reality that|proven fact that} it disappears on shunting the lateral and third ventricles signifies that it as a result of|as a result of} of} hydrocephalic pressure on the mesencephalic tegmentum. If the hydrocephalus becomes arrested, the toddler or youngster is retarded however usually surprisingly verbal. If the head is just moderately enlarged, the child may be able to|could possibly|might be able to} sit however not stand or stand however not stroll. Acute exacerbations of hydrocephalus or an intercurrent febrile illness could cause vomiting, stupor, or coma. The particular options of congenital hydrocephalus related to the Chiari malformation, aqueductal atresia and stenosis, and the Dandy-Walker syndrome are discussed in Chap. Occult Tension Hydrocephalus Here the hydrocephalus becomes evident solely after the cranial sutures have closed (Fig. In some instances the situation offers rise to a normal-pressure hydrocephalus, as discussed under and in Chap. The medical options of occult hydrocephalus and the course of the illness are quite variable. Some instances of arrested hydrocephalus are actually occult in that the illness is unrecognized during life or is found solely by chance imaging of the mind or on postmortem examination. Other signs and indicators are predominantly those of a frontal lobe dysfunction of mentation or of gait. Slowness of mental response (abulia), inattentiveness, distractibility, perseveration, and lack of ability to plan exercise or to sustain any type of advanced cognitive operate are characteristic. The instant responses to verbal and different stimuli are regular, though memory additionally be} barely impaired. Gait deteriorates early in the course of of|in the midst of} hydrocephalus; such deterioration additionally be} current for years before different signs become manifest. The options of gait deterioration are hard to characterize, however the primary features are discussed under, under "Normal-Pressure Hydrocephalus. There is transependymal movement of water that appears as a T2 sign rimming the lateral ventricles. A suck reflex and grasp reflexes of the palms and feet are variably current; plantar reflexes are generally extensor. Clinical Picture of Acute Hydrocephalus Surprisingly little has been written about this syndrome despite its frequency in medical follow. The patient complains of a headache of various severity and sometimes of visual obscuration, could vomit, and then becomes drowsy or stuporous over a period of minutes or hours. Early in the course of, the pupils are regular in measurement and the eyes could rove horizontally; because the ventricles proceed to enlarge, the pupils become miotic, the eyes then cease roving and assume an orthotopic place, or there additionally be} bilateral abducens palsies and limitation of upward gaze. If this situation is left untreated, the pupils ultimately dilate symmetrically, the eyes not respond to oculocephalic maneuvers, and the limbs become flaccid. The latter could pose some risk if spinal fluid is withdrawn quickly, thereby making a pressure gradient between the cerebral and spinal regions. Neuropathologic Effects of Tension Hydrocephalus Ventricular expansion tends to be maximal in the frontal horns, explaining the hydrocephalic impairment of frontal lobe capabilities and of basal ganglionic frontal motor exercise in all forms of hydrocephalus. The central white matter yields to pressure, whereas the cortical grey matter, thalami, basal ganglia, and brainstem constructions stay relatively unaffected. Myelinated fibers and axons are injured, however not to the extent that one may anticipate from the degree of compression; minor degrees of astrocytic gliosis and loss of oligodendrocytes in the affected tissue are current to a lowering extent away from the ventricles and symbolize a hydrocephalic atrophy of the mind. The ventricles are characteristically denuded of ependyma and the choroid plexuses are flattened and fibrotic. Normal-Pressure Hydrocephalus (See also pages one hundred and five to 106) In nonprogressive meningeal and ependymal diseases, hydrocephalus could develop and reach a steady stage. Most usually it takes the type of unsteadiness and impairment of balance, with the greatest problem being encountered on stairs and curbs (Fisher). Weakness and tiredness of the legs are also frequent complaints, although examination discloses no paresis or ataxia. Other patients current with unexplained falls, usually helplessly backward, however on informal inspection the gait could betray no abnormality at all.
Buy generic accupril 10 mg line
The spinoff issues normokalemic periodic paralysis medicine prescription purchase 10mg accupril mastercard, acetazolamide-responsive myotonia medicine and manicures discount accupril 10mg overnight delivery, myotonia fluctuans symptoms 6 days before period discount accupril master card, and myotonia permanens are variants of hyperkalemic periodic paralysis medications dictionary cheap accupril 10mg mastercard. Hyperkalemic Periodic Paralysis the essential features of this illness are episodic generalized weakness of pretty speedy onset and an increase in serum potassium throughout attacks. Weakness appearing after a interval of rest that follows train is especially attribute. This kind of periodic paralysis was first described and distinguished from the more widespread (hypokalemic) type by Tyler and colleagues in 1951. Five years later, Gamstorp described two further families with this disorder and named it adynamia episodica hereditaria. As further examples were reported, it was noted that in a lot of them there were minor degrees of myotonia, which brought the condition into relation with paramyotonia congenita (see further on). Hyperkalemic periodic paralysis was related to a defect in the alpha subunit of the sodium channel gene (Fontaine et al); confirmation that it was a sodium channel disorder adopted shortly thereafter. It is now appreciated that there are distinct variants of hyperkalemic periodic paralysis that breed true. All are related to membrane hyperexcitability due to imperfections in the means of sodium channel inactivation following membrane depolarization as discussed later. Characteristically, the attacks of weakness happen before breakfast and later in the day, notably when resting following train. In the latter case, the weakness seems after 20 to 30 min of becoming sedentary. The patient notes problem that begins in the legs, thighs, and lower again and spreads to the hands, forearms, and shoulders over minutes or more. In extreme circumstances, the attacks could happen every single day; throughout late adolescence and the adult years, when the patient turns into more sedentary, the attacks could diminish and even stop entirely. Indeed, when an attack of paresis is prevented by continuous motion, agency, painful lumps could type in the calf muscle tissue. Some patients with repeated attacks could also be} left with a permanent weakness and wasting of the proximal limb muscle tissue. During the attack of weakness, serum K rises, typically however not always up to as} 5 to 6 mmol/L. With increased urinary excretion of K, the serum K falls and the attack terminates. The test should by no means be undertaken in the presence of an attack of weakness or reduced renal function or in these with diabetes requiring insulin. The treatment of this syndrome is similar as that for paramyotonia congenita, described further on. The disorder can also be|can be} transmitted as an autosomal dominant trait, and the fundamental defect has proved to stem from the same mutation as that of hyperkalemic periodic paralysis of which it could be thought of a variant. In addition, a widespread myotonia, typically coupled with weakness, is induced by exposure to cold. Laboratory Findings In each hyperkalemic periodic paralysis and paramyotonia congenita, the serum K is often above the conventional range throughout bouts of weakness, however paralysis has been observed at levels of 5 meq/L and even lower. Each patient seems to have a critical degree of serum K, which, if exceeded, shall be related to weakness. In vitro studies of muscle from patients with cold-induced stiffness and weakness have shown that as temperature is reduced, the muscle membrane is progressively depolarized to the point where the fibers are inexcitable (Lehmann-Horn et al). In patients with paramyotonia- however not in these with hyperkalemic periodic paralysis- Subramony and colleagues have observed a diminution of the compound muscle action potential in response to the cooling of muscle, settling the argument as to whether or not the two syndromes (hyperkalemic paralysis and paramyotonia) are the same or totally different. Some patients with paramyotonia, like these with certain other types of periodic paralysis, could in later life slowly develop a myopathy that causes persistent weakness. In some circumstances this is sufficiently extreme that it mimics the sample of late-onset limb girdle muscular dystrophy. However, in the case of paramyotonia there are relatively few histologic changes, primarily vacuoles in a number of the} muscle fibers and minimal proof of myofiber degeneration. Treatment Most patients with hyperkalemic periodic paralysis and its variants benefit from prophylactic use of the carbonic anhydrase inhibitor acetazolamide, a hundred twenty five to 250 mg two or 3 times a day.
Buy generic accupril 10 mg
This has suggested to some an imbalance between the satiety heart medications vs medicine generic accupril 10mg free shipping, believed to lie within the ventromedial hypothalamus medicine quotes doctor buy accupril 10mg with visa, and the feeding heart medications in spanish purchase genuine accupril, within the lateral hypothalamus medicine used to stop contractions purchase 10 mg accupril mastercard. It is as though the appetitesatiety mechanism of the feminine hypothalamus have been unstable. The affiliation of anorexia with structural disease involving the appetite facilities has not been established, although the cases reported by Lewin and colleagues and of White and Hain are suggestive. Martin and Reichlin, in citing these uncommon cases, attribute the anorexia and cachexia to lesions of the lateral hypothalamus. A uncommon disorder of infants has been described under the title of "diencephalic syndrome. The causative lesion has normally proved to be a low-grade astrocytoma of the anterior hypothalamus or optic nerve region (Burr et al). As weight is gained over quantity of} weeks, the patient normally turns into more normal in her angle towards consuming and can continue to get well on this routine at residence. Our colleagues report better success with such a routine when imipramine or fluoxetine is added. Others have found these medication to be ineffective except in sufferers with prominent signs of despair. Becker and colleagues emphasised the potentially devastating medical complications to which severely anorectic sufferers are prone and want to|the necessity to} evaluate and deal with these problems on the identical time that nutritional therapy is undertaken. On common, 50 % of sufferers get well fully or almost fully (Steinhausen and Seidel). They either relapse after an initial period of improvement or stay chronically anorectic. Many sufferers are said to lapse into a chronic neurotic state characterized by a persistent preoccupation with food, weight, and dieting. Bulimia may be a|it is a} associated consuming disorder characterized by massive binge consuming adopted by the induction of vomiting or extreme use of laxatives. Indeed, binge consuming is a frequent manifestation of anorexia nervosa, although it additionally occurs as the one, or predominant, consuming disorder. Pope and colleagues reported considerable success in 19 of 20 bulimic sufferers handled with imipramine and adopted for 2 years; the newer antidepressants seem to be equally efficient. From a neurologic perspective, there are four main categories of psychosis: (1) confusional-delirious states, (2) psychoses related to focal or multifocal cerebral lesions, (3) affective issues (manic-depressive and depressive psychoses), and (4) schizophrenia. Depression is perhaps trigger of|the reason for} more grief and misery than some other single disease to which humankind is subject. This view, expressed by Kline almost forty years ago, continues to be shared by everyone within the subject of psychological well being. The quantity of} forms of despair taken together are essentially the most frequent of all psychiatric diseases. In a tertiary general referral hospital, as indicated within the previous chapter, they accounted for an estimated 50 % of psychiatric consultations and 12 % of all admissions to one instructing hospital. In other words, is it mainly a biologic derangement or a response to psychosocial stress? In respect to endogenous despair and manic-depressive psychosis, genetic and neurochemical knowledge cited further on help the kraepelinian view of a disease state. An unfortunate consequence of this view is the belief that an inability to take care of these stresses represents a personal failure of sorts and should inhibit the acceptance of psychiatric assist. Of great consequence for scientific work, depressive states are sometimes related to obscure physical signs. Moreover, the physical signs are incessantly mistakenly attributed to anemia, low blood strain, hypothyroidism, migraine, pressure complications, chronic ache syndrome, chronic infection, emotional problems, fear, and stress. Neurologists are most probably to encounter depressed sufferers who complain of fatigue and weak spot, chronic headache, and difficulty in pondering or remembering. When despair masquerades as a chronic ache or a fatigue state or some other medical situation, it had been referred to as masked despair or depressive equal. Another important reason why all physicians should be knowledgeable about depressive illness in all its types is the danger of suicide, which may be tried and efficiently achieved earlier than the despair is recognized.
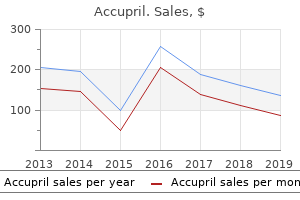
| Comparative prices of Accupril | ||
| # | Retailer | Average price |
| 1 | Winn-Dixie Stores | 109 |
| 2 | SUPERVALU | 821 |
| 3 | Ingles Markets | 557 |
| 4 | Ace Hardware | 562 |
| 5 | Wegman's Food Markets | 352 |
| 6 | Darden Restaurants | 468 |
| 7 | RadioShack | 766 |
Buy cheap accupril 10 mg online
The attribution of those signs to stress of the fetal head on the sacral plexus(es) is conjectural medicine yeast infection buy accupril with paypal. A restricted plexopathy symptoms lactose intolerance 10 mg accupril with visa, occurring after tough vaginal delivery symptoms kennel cough discount accupril 10mg on-line, mainly impairs sensation within the perineum and sphincteric operate (Ismael et al) treatment brown recluse spider bite discount accupril 10 mg with visa. Idiopathic Lumbosacral Plexitis In addition to a diabetic type, an idiopathic neuralgic amyotrophy or lumbosacral plexitis, analogous to the brachial variety, is observed from time to time. After causing widespread unilateral or bilateral sensory, motor, and reflex adjustments in a leg, lumbosacral plexitis may leave the affected person with dysesthesias as troublesome as those that follow herpes zoster (which may also happen at this level). Some patients have had an exploration of the cauda equina (for ruptured disc), even though fact} that|although} lack of sweating and heat of the ft ought to have indicated interruption of autonomic fibers by lesions in peripheral nerves. Diabetic amyotrophy, as a result of} involvement of the lumbar plexus, has a vascular origin, probably inflammatory as mentioned in an earlier part (page 1135), and there are additionally nondiabetic vascular lesions that give rise to equivalent lumbar and upper leg pain and weakness in proximal muscular tissues. The plexus lesions of polyarteritis nodosa, unilateral or bilateral, may also be manifest as a mononeuropathy multiplex. Diabetic mononeuropathy multiplex is mentioned in an earlier half of} this chapter and protruded intervertebral disc syndromes are described in Chap. Lateral Cutaneous Nerve of the Thigh this can be a|it is a} sensory nerve that originates from the second and third lumbar roots and provides the anterolateral facet of the thigh, from the level of the inguinal ligament almost to the knee. The nerve penetrates the psoas muscle, crosses the iliacus, and passes into the thigh by coursing between the attachments of the lateral half of} the inguinal ligament to simply anterior to the anterior superior iliac backbone. Compression (entrapment) may happen at the level the place it passes between the 2 prongs of attachment of the inguinal ligament. Compression of the nerve results in uncomfortable paresthesias and sensory impairment in its cutaneous distribution, a typical condition identified as|often recognized as} meralgia paresthetica (meros, "thigh"). The signs are characteristically worsened in certain positions and after prolonged standing or walking. Most typically the neuropathy is unilateral; Ecker and Woltman discovered solely 20 percent of their circumstances to be bilateral. Most of our patients with meralgia paresthetica request no treatment as soon as} they learn of its benign character. Weight loss and adjustment of restrictive clothing or correction of recurring postures that may compress the nerve are sometimes useful. In one specimen of nerve obtained at operation, we discovered a discrete traumatic neuroma. Hydrocortisone injections at the level of entrapment may have helped in a couple of of} circumstances. Obturator Nerve this nerve arises from the third and fourth and to a lesser extent the second lumbar roots. It provides the adductors of the thigh and contributes to the innervation of the inner and external rotators. The nerve injured by the fetal head or forceps during the course of a tough labor or compressed by an obturator hernia. Femoral Nerve this nerve is formed from the second, third, and fourth lumbar roots. The former provides the pectineus and sartorius muscular tissues and carries sensation from the anteromedial surface of the thigh; the posterior division provides the motor innervation to the quadriceps and the cutaneous innervation to the medial facet of the leg from the knee to the inner malleolus. The adductor of the thigh (innervated by the obturator nerve) is spared, distinguishing femoral neuropathy from an L3 radiculopathy. Usually that is the result of|the results of} improper placement of retractors, which may compress the nerve immediately or indirectly by undue stress on the psoas muscle. Bleeding into the iliacus muscle or the retroperitoneum, observed in patients receiving anticoagulants and in hemophilia patients, is a comparatively widespread cause of isolated femoral neuropathy (Goodfellow et al). The presenting symptom of iliacus hematoma is pain within the groin spreading to the lumbar area or thigh, in response to which the affected person assumes a attribute posture of flexion and lateral rotation of the hip. A palpable mass within the iliac fossa and the indicators of femoral nerve compression (quadriceps weakness and lack of knee jerk) follow in a day or two. Sciatic Nerve this nerve is derived from the fourth and fifth lumbar and first and second sacral roots, for which purpose a ruptured disc at any of those levels may simulate sciatic neuropathy (sciatica). The sciatic nerve provides motor innervation to the hamstring muscular tissues and all of the muscular tissues under the knee by way of its two divisions, the tibial and peroneal nerves (see later); the sciatic nerve conveys sensory impulses from the posterior facet of the thigh, the posterior and lateral aspects of the leg, and the whole sole.
Buy accupril mastercard
In recent years treatment 1st 2nd degree burns cheap accupril online, quantity of|numerous|a selection of} necessary observations have been made concerning the mode of transmission and modulation of ache impulses within the dorsal horn and brainstem symptoms 5 days before missed period 10mg accupril overnight delivery. Also symptoms xanax treats buy generic accupril 10 mg on-line, A- ache afferents medicine man dr dre generic accupril 10 mg visa, when stimulated, launch several of} neuromodulators that play a role within the transmission of ache sensation. Slower neurotransmission by C neurons includes different substances, of which the most important is the 11 amino acid peptide identified as|often recognized as} substance P. In animals, substance P has been proven to excite nociceptive dorsal root ganglion and dorsal horn neurons; moreover, destruction of substance P fibers produces analgesia. Thus, opiates have been famous to lower substance P; on the similar time, flexor spinal reflexes, which are evoked by segmental ache, are lowered. The topic of ache modulation by opiates and endogenous morphinelike substances is elaborated additional on. The principal bundle of those axons decussates within the anterior spinal commissure and ascends within the anterolateral fasciculus because the spinothalamic tract to terminate in several of} brainstem and thalamic buildings (Fig. It is of scientific consequence that the axons carrying ache impulses from every dermatome decussate one to three segments above the extent of root entry. For this reason, a discrete lesion of the lateral spinal wire creates a lack of ache and thermal sensation of the contralateral trunk, the dermatomal level of which is two to three segments below that of the spinal wire lesion. Most of the fibers terminate inside the segment of their entry into the wire; some lengthen ipsilaterally to one or two adjoining rostral and caudal segments; and some project, through the anterior commissure, to the contralateral dorsal horn. The cytoarchitectonic studies of Rexed within the cat (the similar organization pertains in primates and doubtless in humans) have proven that secondorder neurons, the websites of synapse of afferent sensory fibers within the dorsal horn, are organized in a series of six layers or laminae (Fig. Spinal wire in transverse section, illustrating the course of the afferent fibers and the most important ascending pathways. Transverse section by way of a cervical segment of the spinal wire, illustrating the subdivision of the gray matter into laminae according to Rexed and the entry and termination of the principle sensory fibers. One such group of fibers initiatives on to the reticular core of the medulla Face and midbrain and then to the medial and intralaminar nuclei of the thalamus; this group of fibers is referred Thalamus to because the spinoreticulothalamic or paleospinothalamic pathway. At the extent of the medulla, these fibers synapse within the nucleus gigantocellularis; extra rostrally, Ventral they connect with nuclei of the parabrachial area, posterolateral midbrain reticular formation, periaqueductal grey nucleus of thalamus matter, and hypothalamus. There can also be|can be} a third, direct spinohypothalamic pathMedial lemniscus way within the anterolateral fasciculus. Nucleus of the conduction of diffuse, poorly localized ache funiculus gracilis arising from deep and visceral buildings (gut, periNucleus of osteum) has been ascribed to these pathways. Offshoots from the ascending anterolateral fasciculus (spinothalamic tract) to nuclei tensity of the noxious stimulus. Also, the pathways within the medulla, pons, and mesencephalon and nuclear terminations of the tract are indicated. One of those is a longitudinal polysynaptic bundle of the cells of termination of cutaneous nociceptive stimuli and the small myelinated fibers within the center of the dorsal horn (the dorsal cells of origin of ascending spinal afferent pathways have all been intracornual tract); one other consists of axons of lamina I cells that obtained from studies in animals (including monkeys). Information about this pathway in Thalamic Terminus of Pain Fibers people has been derived from the study of postmortem material and from the examination of sufferers subjected to anterolateral corThe direct spinothalamic fibers separate into two bundles as they dotomy for intractable ache. The medial contingent terminates mainly in opposite aspect of the physique, extending to a level two or three segthe intralaminar complex of nuclei and within the nucleus submedius. The cortical representation permits for accurate localization of the site of origin of a painful stimulus however the notion that thalamic projections terminate solely in this area is an oversimplification. However, cerebral evoked potentials and elevated cerebral blood flow (by positron emission tomography studies) have been demonstrated within the thalamus and pre- and postcentral gyri of sufferers undergoing rectal balloon distention (Silverman et al; and Rothstein et al). Spinal wire displaying the segmental association of nerve fibers within main tracts. On the left aspect are indicated the "sensory modalities" that seem to be mediated by the two main ascending pathways. Projections from the dorsal column nuclei, which have a modulating influence on ache transmission, are mainly to the ventrobasal and ventroposterior group of nuclei. Each of the 4 thalamic nuclear teams that receives nociceptive projections from the spinal wire has a definite cortical projection, and each is assumed to play a special function in ache sensation (see below). In general, neurophysiologic evidence indicates that as one ascends from peripheral nerve to spinal, medullary, mesencephalic, thalamic, and limbic levels, the predictability of neuron responsivity to noxious stimuli diminishes. Thus it comes as no surprise that neurosurgical procedures for interrupting afferent pathways become much less and fewer profitable at progressively higher levels of the brainstem and thalamus. Of great significance was the invention of a system of descending fibers and way stations that modulate activity in nociceptive pathways.
Accupril 10 mg sale
Somnambulism within the adult 7 medications that cause incontinence generic accupril 10mg without a prescription, as within the youngster medications kidney damage purchase accupril mastercard, is usually a|could be a} purely passive occasion unaccompanied by fear or other indicators of emotion treatments yeast infections pregnant buy 10mg accupril fast delivery. More incessantly medicine park oklahoma 10 mg accupril with visa, nonetheless, the assault is characterized by frenzied or violent habits associated with fear and tachycardia, like that of a night terror and typically with self-injury. The finding of normal sleep patterns on polysomnography distinguishes these attacks from complicated partial seizures. Some sufferers reply higher to a mix of clonazepam and phenytoin or to flurazepam (Kavey et al). Half-waking somnambulism, or sleep automatism, is a closely associated dysfunction in which an adult, half-roused from sleep, goes by way of a reasonably complicated collection of purposeful but inappropriate acts, similar to going to a window, opening it, and searching, but afterward recalling the episode only vaguely and partially. It is characterized by attacks of vigorous and infrequently harmful motor exercise accompanied by vivid goals (Mahowald and Schenck). The episodes are of various frequency, occurring as soon as} every week or two or a number of} occasions nightly. The attribute features are angry speech with shouting, violent exercise with harm to self and bedmate, a very high arousal threshold, and the detailed recall of a nightmare of being attacked and combating back or attempting to flee. Polysomnographic recordings throughout these episodes have disclosed augmented muscle tone. The uncommon look of this dysfunction with pontine infarctions has been mentioned (page 340). These episodes could be suppressed by the administration of clonazepam in doses of zero. Discontinuation of medication, even after years of efficient control, has resulted in relapse. The look of such a seizure decided by} the phase of the seizure in which the affected person occurs to be when first noticed. If the nocturnal seizure is unobserved, the only indication of it might be disheveled bedclothes, a number of} drops of blood on the pillow from a bitten tongue, moist bed linen from urinary incontinence, or sore muscle tissue. Or the incidence of a seizure additionally be} betrayed only by confusion or headache, the frequent aftermaths of a serious generalized seizure. Rarely, a affected person might die in an epileptic seizure throughout sleep, typically from smothering within the bedclothes or aspirating vomitus or for some obscure purpose (possibly respiratory or cardiac dysrhythmia). These accidents and similar ones in awake epileptics account for the higher mortality price in epileptics than in nonepileptics. Rarely, epilepsy occurs along side of} night time terrors and somnambulism; the query then arises whether or not the latter disorders represent postepileptic automatisms. Excessive Sleep (Hypersomnia) and Reversal of Sleep-Wake Rhythm Encephalitis lethargica, or von Economo "epidemic encephalitis," the outstanding illness that appeared on the medical horizon as a pandemic following World War I, supplied variety of the} most dramatic instances of pathologic somnolence. In reality, protracted sleep lasting for days to weeks was such a distinguished symptom of this illness that it was called sleeping illness. The affected person appeared to be in a state of continuous sleep, or somnosis, and could be be} saved awake only by constant stimulation. Although the infective agent was by no means isolated, the pathologic anatomy was absolutely divulged by many excellent research, all of which demonstrated a destruction of neurons within the midbrain, subthalamus, and hypothalamus. Patients who survived the acute phase of the illness usually had problem in re-establishing their normal sleep-wake rhythm. As the somnolence disappeared, some sufferers exhibited a reversal of the traditional pattern, tending to sleep by day and stay awake at night time; many of them additionally developed a parkinsonian syndrome months or years later. Possibly the hypersomnia was associated to destruction or practical paralysis of dopamine-rich neurons within the substantia nigra, resulting in overactivity of the raphe (serotonergic) neurons. Hypersomnia a manifestation of trypanosomiasis, the frequent explanation for "sleeping illness" in Africa, and of other diseases localized to the mesencephalon and the floor and partitions of the third ventricle, as indicated earlier in this chapter. Small tumors in this space have been associated with arterial hypotension, diabetes insipidus, hypo- or hyperthermia, and protracted somnolence lasting many weeks. Traumatic and vascular lesions and other diseases affecting the mesencephalon might have an identical impact.
Discount 10 mg accupril mastercard
The solely neurologic residua have been a gentle defect in retentive memory and areas of decreased attenuation within the pallidum bilaterally (arrows) medicine man pharmacy purchase 10 mg accupril otc. This remedy reduces the incidence of cognitive sequelae from forty six to 25 p.c based on medications names cheap accupril 10 mg free shipping a trial performed by Weaver and colleagues medicine quetiapine cheap accupril 10 mg fast delivery. High-Altitude (Mountain) Sickness Acute mountain sickness is one other special type of cerebral hypoxia medications valium buy generic accupril online. Headache, anorexia, nausea and vomiting, weak point, and insomnia seem at altitudes above 8000 ft; on reaching larger altitudes, there additionally be} ataxia, tremor, drowsiness, mild confusion and hallucinations. At 16,000 ft, based on Griggs and Sutton, 50 p.c of people develop asymptomatic retinal hemorrhages, and it has been instructed that such hemorrhages additionally happen within the cerebral white matter. With more extended exposure at these altitudes or with further ascent, affected people suffer psychological impairment which will progress to coma. Hypoxemia at high altitude is intensified during sleep, as air flow usually diminishes. Oxygen supplementation is, in fact, used cautiously in these sufferers have the ability to} keep away from suppressing respiratory drive- marginally compensated sufferers treated with extreme oxygen have lapsed into coma. Treatment of coronary heart failure, phlebotomy to reduce the viscosity of the blood, and antibiotics to suppress pulmonary an infection additionally be} necessary. Often these measures result in a surprising diploma of enchancment, which can be maintained for months or years. Unlike pure hypoxic encephalopathy, extended coma because of of} hypercapnia is relatively rare and in our experience has not led to irreversible mind injury. Papilledema and jerky, intermittent lapses of sustained muscular contraction (asterixis) are important diagnostic features. If aminophylline is run for the remedy of the underlying pulmonary airway disease, there additionally be} a tendency for seizures. The syndrome is apt to be mistaken for a mind tumor, confusional psychosis of other sort, or a disease causing chorea or myoclonus. In the last occasion, hypercapnia must be distinguished from other metabolic diseases presenting as chronic extrapyramidal syndromes, as described later on this chapter. The mind is the only organ besides the center that suffers severe useful and structural impairment beneath circumstances of severe hypoglycemia. It is known that hypoglycemia reduces O2 uptake and will increase cerebral blood circulate. The levels of several of} mind phospholipid fractions decrease when animals are given giant doses of insulin. However, the suggestion that hypoglycemia results in a rapid depletion and inadequate production of high-energy phosphate compounds has not been corroborated; another glucose-dependent biochemical process must be implicated. Etiology the most common causes of hypoglycemic encephalopathy are (1) unintended or deliberate overdose of insulin or an oral diabetic agent; (2) islet cell insulin-secreting tumor of the pancreas; (3) depletion of liver glycogen, which often follows a protracted alcoholic binge, starvation, or some type of acute liver disease such as acute nonicteric hepatoencephalopathy of childhood (Reye syndrome); (4) glycogen storage disease of infancy; and (5) an idiopathic hypoglycemia within the neonatal interval and, less often, of infancy. Moderate degrees of hypoglycemia (50 mg/dL) additionally be} noticed with chronic renal insufficiency (Fisher et al). In the previous, hypoglycemic encephalopathy was a not rare complication of "insulin shock" remedy for schizophrenia. Clinical Features the preliminary symptoms seem when the level of blood glucose has descended to about 30 mg/dL- nervousness, hunger, flushed facies, sweating, headache, palpitation, trembling, and nervousness. These steadily give method to confusion and drowsiness and infrequently to excitement, overactivity, and bizarre or combatative habits. Many of the early and mild symptoms relate to adrenal and sympathetic overactivity; subsequently a number of the} manifestations additionally be} muted in diabetic sufferers with neuropathy. In the subsequent stage, pressured sucking, grasping, motor restlessness, muscular spasms, and decerebrate rigidity happen, in that sequence. Rarely there are focal cerebral deficits, the pathogenesis of which stays unexplained; based on Malouf and Brust, hemiplegia, corrected by intravenous glucose, was noticed in 3 of a hundred twenty five sufferers who introduced with symptomatic hypoglycemia. Blood glucose levels of approximately 10 mg/dL are associated with deep coma, dilatation of pupils, pale skin, shallow respiration, sluggish pulse, and hypotonia of limb musculature- the "medullary phase" of hypoglycemia. If glucose is run before this degree has been attained, the affected person can be restored to normalcy, retracing the aforementioned steps in reverse order. However, as soon as} the medullary phase is reached, and particularly if it persists for a time before the hypoglycemia is corrected by intravenous glucose or spontaneously as a result of|because of|on account of} the gluconeogenic activities of the adrenal glands and liver, restoration is delayed for a interval of days or weeks weeks|days or even weeks} and additionally be} incomplete as famous under. A giant dose of insulin, which produces intense hypoglyce- Hypoglycemic Encephalopathy this condition is now relatively rare but is a vital reason for confusion, convulsions, stupor, and coma; as such, it merits separate consideration as a metabolic dysfunction of the mind.
Buy line accupril
The authors have grouped this disease with the other inherited choreas (Huntington disease conventional medicine purchase accupril with mastercard, neuroacanthocytosis medications in pregnancy buy generic accupril on line, familial calcification of basal ganglia treatment programs discount accupril 10 mg overnight delivery, Hallervorden-Spatz disease symptoms 7 days after implantation 10mg accupril visa, acanthocytic chorea, dentatorubrothalamic atrophy). Most of the above-mentioned ailments are presently classified as degenerative and are discussed in Chap. Of the quantity of} kinds of late-onset leukodystrophy, some are of unquestionable metabolic origin and others are of unsure standing. As emphasized earlier, all differ from the cerebral gray matter ailments (poliodystrophies), which have a special mode of presentation- seizures, myoclonus, chorea, choreoathetosis, and tremor being prominent. The syndrome of progressive spasticity and rigidity with spastic dysarthria and pseudobulbar palsy poses another tough diagnostic problem. In addition, unusual postures and a more plastic sort of rigidity may occur, consistent with with} an extrapyramidal situation. Furthermore, the mix of lowered or absent tendon reflexes and Babinski signs, signifying a combination of corticospinal and peripheral nerve lesions, is very attribute of metachromatic leukoencephalopathy, adrenomyeloneuropathy, or subacute mixed degeneration of the spinal twine (vitamin B12 deficiency). Such combinations, with mental backwardness and dementia, characterize the gentle and late types of metachromatic leukodystrophy. The leukodystrophies that turn into obvious solely in later life pose another problem- the medical and radiologic differentiation from cerebral types of a number of} sclerosis. In circumstances of early onset, in which myelin has but to be normally fashioned, the metabolic disturbance may lead to hypomyelination. In figuring out the metabolic ailments of myelin, one is helped by the relative symmetry and regular development of the medical signs; the early onset of cognitive impairment (which is uncharacteristic of a number of} sclerosis); and the symmetrical and massive degeneration of the cerebral white matter (in distinction to the asymmetrical and infrequently a number of} lesions of demyelinative disease). Differentiation from cerebral gliomatosis, brain lymphoma, and progressive multifocal leukoencephalopathy, all affecting deep cerebral or white matter constructions, presents much less issue. It is transmitted as an X-linked recessive trait with an incidence of 1 in 20,000 male births. The trendy classification of the disease categorizes it as a dysfunction of peroxisomes, subcellular organelles containing quite a few enzymes. This peroxisomal assignation connects adrenoleukodystrophy with Zellweger and Refsum disease. The onset is usually between 4 and eight years, generally later; in the most common form of this dysfunction, solely males are affected with the complete syndrome (women carriers may display a particular myelopathy discussed further on). The signs of both the adrenal insufficiency or the cerebral lesion may be the first to seem. In the case of Siemerling and Creutzfeldt, the primary recorded instance of this dysfunction, bronzing of the pores and skin of the palms appeared at 4 years of age; quadriparesis, with dysarthria and dysphagia. In personally noticed circumstances, the primary abnormalities appeared at 9 to 10 years and took the form of episodic vomiting, decline in scholastic performance, and alter in persona, with foolish, inappropriate giggling and crying. After a time, severe vomiting and even an episode of circulatory collapse occurred, following which the gait became unsteady and arms ataxic, with an action or intention tremor. The late phases were marked by bilateral hemiplegia (at first asymmetrical), pseudobulbar paralysis, blindness, deafness, and impairment of all larger cerebral capabilities. We are caring for two adult men in whom the cerebral signs have been gentle, allowing for high-level cognitive achievement, albeit with peculiarities of persona, and with gentle spastic gait, urinary issue, testicular insufficiency, and baldness. In every household there was a male sibling who died in childhood, ostensibly of adrenal insufficiency. In their patients, evidence of adrenal insufficiency had been present since early childhood, however solely within the third decade of life did a progressive spastic paraparesis and a relatively gentle polyneuropathy develop. It should be noted that the spasticity is often asymmetrical, and the gait may have an ataxic element. This neurologic picture, in gentle type and without adrenal insufficiency, additionally be|can be} the style in which the disease may present in feminine carriers of the gene abnormality (see below). A progressive degeneration of cerebral white matter in younger males, often with cortical blindness- the classic sort, accounting for half of all circumstances (Fig. An intermediate type in juvenile or younger adult males with cerebral and spinal involvement (5 percent of cases) three. A progressive spinal twine tract degeneration in adult males (25 percent of cases) 4. A persistent gentle, nonprogressive spastic paraparesis in heterozygous feminine carriers (10 percent of cases) 5. Familial cases of Addison disease without neurologic involvement in males (10 percent) 6. Moser found cerebral types alone in 30 percent, adrenomyeloneuropathy alone in 20 percent, and mixed childhood cerebral and myelopathic types within the remaining half.
References:
- https://academic.oup.com/DocumentLibrary/Bjaed/BJA%20Education%20December%202015%20CME.pdf
- http://www.medicalsciencejournal.com/download/1338/5-3-16-634.pdf
- https://www.who.int/classifications/icd/ICD-10_2nd_ed_volume2.pdf