
Tizanidine
"Buy line tizanidine, spasms while pregnant".
By: D. Anktos, MD
Clinical Director, Northeast Ohio Medical University College of Medicine
Buy tizanidine online
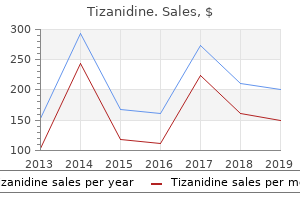
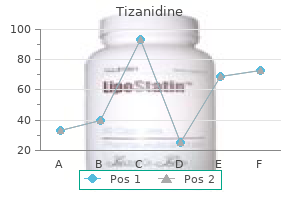
Figure thirteen-3 depicts typical development curves for 4 courses of decreased linear development muscle relaxant video order tizanidine with paypal. In congenital pathologic short stature muscle relaxant guidelines cheap tizanidine 4 mg amex, an toddler is born small and development gradually tapers off throughout infancy spasms headache discount tizanidine online amex. In constitutional development delay muscle relaxant 2632 buy 4mg tizanidine with mastercard, weight and peak lower close to the top of infancy, parallel the norm via middle childhood, and accelerate toward the top of adolescence. In familial short stature, each the toddler and the parents are small; development runs parallel to and just below the normal curves. Growth charts can verify an impression of obesity if the load for peak exceeds one hundred twenty% of the usual (median) weight for peak. Measurement of the triceps, subscapular, and suprailiac skinfold thickness can be utilized to estimate adiposity; considerable experience is required for accuracy. Other strategies of measuring fats, corresponding to hydrodensitometry, bioelectrical impedance, and total body water measurement are used in analysis, but not in scientific analysis. The head and trunk are relatively large at start, with progressive lengthening of the limbs throughout improvement, particularly throughout puberty. The lower body segment is defined as the length from the symphysis pubis to the floor, and the upper body segment is the height minus the lower body segment. The ratio of upper body segment divided by lower body segment (U/L ratio) equals roughly 1. Higher U/L ratios are attribute of short-limb dwarfism or bone problems, corresponding to rickets. Skeletal Maturation Reference standards for bone maturation facilitate estimation of bone age (see Table 8-3). Bone age correlates properly with stage of 6 pubertal improvement and can be helpful in predicting adult peak in early- or late-maturing adolescents. In familial short stature, the bone age is normal (corresponding to chronological age). In constitutional delay, endocrinologic short stature, and undernutrition, the bone age is low and corresponding to the height age. Skeletal maturation is linked extra closely to sexual maturity ranking than to chronological age. Dental improvement consists of mineralization, eruption, and exfoliation (Table thirteen-3). Initial mineralization begins as early as the 2nd trimester (imply age for central incisors, 14 wk) and continues via 3 yr of age for the first (deciduous) tooth and 25 yr of age for the permanent tooth. Eruption begins with Dental Development 2 imply 2 Figure thirteen-3 Height-for-agecurvesofthefour generalcausesofproportionalshortstature: postnatalonsetpathologicshortstature, constitutionalgrowthdelay,familialshortstature, andprenatalonsetshortstature. Eruption of the permanent tooth could observe exfoliation instantly or could lag by 4-5 mo. The timing of dental improvement is poorly correlated with other processes of development and maturation. Common causes embody hypothyroid, hypoparathyroid, familial, and (the most common) idiopathic. Individual tooth could fail to erupt because of mechanical blockage (crowding, gum fibrosis). Causes of early exfoliation embody histiocytosis X, cyclic neutropenia, leukemia, trauma, and idiopathic components. Nutritional and metabolic disturbances, extended sickness, and sure medications (tetracycline) commonly end in discoloration or malformations of the dental enamel. Structural Growth Virtually each organ and physiologic process undergoes a predictable sequence of structural or functional adjustments, or each, throughout improvement. Reference values for developmental adjustments in a wide variety of techniques (pituitary and renal function, electroencephalogram, and electrocardiogram) have been printed. Hochberg Z, Albertsson-Wikland K: Evo-devo of infantile and childhood development, Pediatr Res 64:2�7, 2008.
Buy line tizanidine
Current proof means that dexamethasone added to the routine decreases long-term problems of the infection spasms prednisone purchase tizanidine pills in toronto. Other infections causing coma (Chapter 5) must Adjust Body Temperature Several metabolic and structural abnormalities result in spasms treatment generic 2 mg tizanidine with amex both hyperthermia or hypothermia spasms with fever trusted tizanidine 4mg, and these states may exacerbate abnormalities of cerebral metabolism back spasms 35 weeks pregnant tizanidine 4 mg. Significant hypothermia (beneath 348C) can result in pneumonia, cardiac arrhythmias, electrolyte issues, hypovolemia, metabolic acidosis, impaired coagulation, and thrombocytopenia and leukopenia. Administer Specific Antidotes Many patients entering an emergency room in coma are suffering from drug overdose. Empiric addition of amoxicillin is indicated for meningitis attributable to Listeria monocytogenes. Continuation or change of antibiotics is guided by the results of cerebrospinal fluid evaluation, blood tradition, bacterial sensitivity to antibiotics, and scientific status of the patient. Most drug overdoses are best treated by the supportive measures thought of in a subsequent part. Because these patients have ingested a number of brokers, particular antagonists are often not useful. This drug have to be used with nice care, as a result of in a patient physically dependent on opioids, the drug may cause acute withdrawal symptoms requiring opioid therapy. One should use the minimum quantity necessary to establish the diagnosis by pupillary dilation and reverse the comatose state. Benzodiazepine overdose can be treated with flumazenil, a particular competitive benzodiazepine receptor antagonist41 (zero. Approach to Management of the Unconscious Patient 317 Table 7�three Specific Antidotes for Agents Causing Delirium and Coma Antidote Naloxone Flumazenil Physostigmine Fomepizole Glucagon Hydroxocobalamin Octreotide Indication Opioid overdose Benzodiazepine overdose Anticholinergic overdose ( Tricyclic overdose Cyanide overdose Sulfonylurea hypoglycemia mary medication have failed. Corneal erosions can happen within 4 to 6 hours if the eyes of comatose patients remain partially or absolutely opened. To forestall such changes, lubricate the eyes with a lubricating artificial tears ointment every 4 hours45 or apply a polyethylene corneal bandage. A safer approach is to drip sterile saline onto the cornea from a distance of 4 to 6 inches. The hyperactivity is distressing to patients and household and may result in self-damage. Sedative dosages of drugs should be averted until the diagnosis is evident and one is definite that the issue is metabolic quite than structural. Agitation can be managed by keeping the patient in a lighted room and asking a relative or employees member to sit on the bedside and discuss reassuringly to the patient. The examination of the unconscious patient is roofed in detail in Chapter 2, however a quick reprise is included here with emphasis on the elements that must be covered shortly while initiating therapy in a scientific setting. The historical past should, to whatever extent possible, be obtained from relatives, associates, paramedics, or sometimes even the police. Coma of sudden onset in a beforehand healthy patient often seems to be self-induced drug poisoning, subarachnoid hemorrhage, head trauma, or, in older individuals, brainstem hemorrhage or infarction. In the final physical examination, after assessing and dealing with abnormalities of important signs, look for proof of trauma or signs that may recommend an acute or persistent systemic medical illness or the ingestion of self-administered medication. Evaluate nuchal rigidity, however take care first to be sure that the cervical backbone has not been injured. Table 7�4 outlines the scientific neurologic features that provide essentially the most useful data in making a categoric diagnosis. Pupillary Reactions Pupillary reactions to an intense flashlight beam are evaluated for both eyes, and the higher response is recorded; use a hand lens or the plus 20 lens on the ophthalmoscope to consider questionable responses. Record pupillary diameters and observe the presence of any somatic third nerve paresis. Verbal Responses the best response, oriented speech, implies awareness of self and the environment. The patient knows who he or she is, where he or she is, why he or she is there, and the yr, season, and month. Confused dialog describes conversational speech with syntactically correct phrases however with disorientation and confusion within the content. Incomprehensible speech refers to the production of word-like mutterings or groans. Spontaneous Eye Movement the best response is spontaneous orienting eye movements in which the patient appears towards environmental stimuli.
Syndromes
- Large and full bladder
- Scarring of lung tissue
- Over time, however, nasal polyps often return.
- Electrical signals travel in new or different pathways through the heart
- Excessive thirst
- Fainting or feeling light-headed
Buy tizanidine 4 mg with mastercard
Although in some cases it seems that the syndrome happens after just one stroke spasms left shoulder blade tizanidine 4mg fast delivery, further investigation typically reveals evidence of a preexisting lesion on the contralateral aspect muscle relaxant drug list buy tizanidine overnight, a lesion which had been clinically "silent" (Besson et al muscle relaxant vs analgesic discount 2mg tizanidine amex. Of the neurodegenerative problems associated with pseudobulbar palsy muscle relaxant radiolab discount tizanidine online master card, probably the most outstanding is amyotrophic lateral sclerosis, whereby approximately one-half of patients are eventually so affected (Gallagher, 1989). Of the miscellaneous causes, cerebral tumors which bilaterally compress or invade the brainstem are notably necessary. Course the general course of the syndrome reflects the course of the etiologic dysfunction. The look of dysphagia, nevertheless, is an ominous signal, carrying, because it does, the chance of aspiration. Among the tricyclics, each amitriptyline (in doses of fifty�75 mg) and nortriptyline (in doses up to a hundred mg) are efficient, with nortriptyline typically better tolerated. Kl�ver�Bucy Syndrome Definition In 1939, Kl�ver and Bucy (1939) noted some striking behavioral changes in monkeys which had been subjected to bilateral Chapter 33 � Mental Disorders Due to a General Medical Condition 407 temporal lobectomy, and in so doing described the syndrome that now bears their names. The full syndrome is characterised by hypermetamorphosis (excessive tendency to take discover and attend and react to each visual stimulus), agnosia, hyperorality, emotional placidity and hypersexuality. The first example demonstrates hypersexuality, hyperorality, agnosia and emotional placidity. The patient was a 31-12 months-old lady, who, after recovering from a herpes simplex encephalitis, "made inappropriate sexual advances to feminine attendants, each manually and orally. At house, she was continuously chewing and swallowing, and all objects inside attain had been placed in her mouth. Her have an effect on was characterised by passivity and a pet-like compliance with those attending her" (Lilly et al. The second example supplies examples of hypermetamorphosis, hyperorality, agnosia and hypersexuality. He placed many objects in his mouth and sometimes ate soil from plant containers. He additionally placed objects in his mouth, chewed on tissue paper, and attempted to drink from his urine container" (Nakada et al. Of the miscellaneous causes, an ictal Kl�ver�Bucy syndrome is usually recommended by its exquisitely paroxysmal onset and by the prevalence of other signs typical for a posh partial seizure, such as confusion, and a postictal Kl�ver�Bucy syndrome by the historical past of an instantly previous generalized seizure. Adrenoleukodystrophy, the last in the record, is a particularly rare explanation for the Kl�ver�Bucy syndrome. The differential rests on the presence or absence of pressured speech and activity, findings typical of mania however absent in the Kl�ver� Bucy syndrome. Epidemiology and Comorbidity the total Kl�ver�Bucy syndrome is, overall, rare; in dementia clinics, nevertheless, full or partial Kl�ver�Bucy syndromes are generally seen. Course the course depends on the underlying trigger; in some cases, the syndrome itself may have a deadly end result, as in the following scientific vignette. Etiology and Pathophysiology the various causes of the Kl�ver�Bucy syndrome are listed in Table 33. The mechanism of such bilateral damage in the case of precipitants is pretty simple. In persistent cases, neuroleptics have been reported to be useful; there are, nevertheless, no managed research. Ishii N, Nishihara Y and Imamura T (1986) Why do frontal lobe signs predominate in vascular dementia with lacunes Rodin E and Schmaltz S (1984) the Bear�Fedio character inventory and temporal lobe epilepsy. Anderson G, Vestergaard K and Lauritzen L (1994) Effective treatment of poststroke depression with the selective serotonin reuptake inhibitor citalopram. Since a analysis of substance dependence preempts a analysis of abuse, tolerance, withdrawal and compulsive use are typically not present in people with a analysis of substance abuse. A maladaptive sample of substance use resulting in clinically vital impairment or misery, as manifested by one (or more) of the following, occurring inside a 12-month period: (1) recurrent substance use resulting in a failure to fulfill major position obligations at work, college, or house. The signs have by no means met the factors for substance dependence for this class of substance. Substance Intoxication Substance intoxication is a reversible substance-particular syndrome with maladaptive behavioral or psychological changes creating throughout or shortly after utilizing the substance. Recent use could be documented by a historical past or toxicological screening of physique fluids (urine or blood).
Cheap 2 mg tizanidine with visa
After acquiring all of the required info muscle relaxant blood pressure cheap tizanidine express, the catheter is removed and a vascular closure system could also be placed muscle relaxant tl 177 purchase tizanidine canada. A chemical vascular closure system designed to seal the arterial puncture is commonly placed spasms in your sleep tizanidine 2mg line. Tell the patient that during the injection she or he may experience a severe hot flush spasms and spasticity order line tizanidine. Instruct the patient to report any indicators of numbness, tingling, pain, or loss of function within the concerned extremity. C 220 cardiac catheterization Instruct the patient that the check shall be reviewed by the cardiologist and the results shall be out there in 1 or 2 days. It could also be carried out after a coronary ischemic event to evaluate coronary patency or coronary heart muscle function. This scan may be carried out at relaxation or with exercise such as treadmill or bicycling (myocardial nuclear stress testing). Vasodilators (dipyridamole, adenosine, and regadenoson) or chronotropic agents (dobutamine) are generally used. Regadenoson is the most recent A2A adenosine receptor agonist that instigates coronary vasodilatation. Technetium agents such as tetrofosmin and sestamibi (isonitrile) are actually extra generally used. At relaxation, a coronary stenosis must exceed ninety% of the traditional diameter earlier than blood move is impaired enough to see it on the perfusion scan. Often, stenosis or coronary obstruction is famous by a standard resting perfusion scan adopted by stress perfusion scan 222 cardiac nuclear scan that demonstrates cold spots appropriate with decreased coronary perfusion. Myocardial perfusion scans may be synchronized by gating the pictures with the cardiac cycle and thereby permitting the visualization and evaluation of cardiac muscle function. Most occasions, nuclear myocardial scans embody both perfusion and gated wall movement images. Cardiac ejection fraction, the end-systolic quantity of the left ventricle, may be calculated. This is used within the initial evaluation of cardiac function and subsequently to monitor therapy designed to improve cardiac function. Patients with cardiomyopathies (ischemic, infiltrative, inflammatory), cardiac transplant, or drug-induced cardiac muscle toxicity (from doxorubicin or Herceptin) require frequent evaluation of ventricular ejection fraction. Instruct the patient that a brief fasting period could also be required, particularly when using sestamibi or tetrofosmin. Depending on the type of nuclear myocardial scan, every scanning protocol is completely different. Depending on the radionuclide used, scanning is carried out quarter-hour to four hours later. If a single gamma digicam is used, the patient is placed in a supine position, then could also be repositioned to the lateral position or in the right and left indirect positions. In some departments, the detector may be rotated around the patient, who remains within the supine position. The gamma ray scanner data the picture of the heart, and a picture is immediately developed. For an exercise stress check, additional radionuclide is injected throughout exercise when the patient reaches a most coronary heart fee. If an isonitrile stress check is needed, the radionuclide materials is injected and a scan carried out 30 to 60 minutes later for the resting part. After Inform the patient that as a result of solely tracer doses of radioisotopes are used, no precautions have to be taken against radioactive exposure to personnel or family. Instruct the patient to drink fluids to assist within the excretion of the radioactive substance. Type of check Electrodiagnostic; nuclear Normal findings Patient capable of obtain and keep maximal C Test explanation and related physiology Stress testing is used within the following conditions: � To evaluate chest pain in a patient suspected of having coronary illness � To decide the bounds of safe exercise throughout a cardiac rehabilitation program or to help sufferers with cardiac illness in sustaining good bodily fitness � To detect labile or exercise-related hypertension � To detect intermittent claudication in sufferers with suspected vascular occlusive illness within the extremities � To evaluate the effectiveness of therapy in sufferers who take antianginal or antiarrhythmic drugs � To evaluate the effectiveness of cardiac intervention. In stress testing, the heart is stressed indirectly after which evaluated during the stress. Chemical stress testing strategies have gotten extra generally used due to their safety and increased accuracy.
Buy tizanidine 4 mg
The fee of deaths from drug overdose dropped considerably in France after buprenorphine was introduced for therapy of drug dependence muscle relaxant no drowsiness generic 4mg tizanidine. The one exception was overdoses of buprenorphine in combination with benzodiazepines where deaths had been noticed spasms caused by anxiety purchase tizanidine with amex. This has led to an exaggerated concern that buprenorphine is contraindicated in patients who use benzodiazepines spasms gums generic tizanidine 2mg amex. For patients using benzodiazepines at common muscle relaxant on cns order tizanidine cheap, modest doses, which is the most typical sample even among opiate addicts, buprenorphine is safe. Patients who take giant doses or binges of benzodiazepines are at risk for overdose in combination with quite a lot of different medicine, including buprenorphine, and alcohol. It is probably going that the chance of overdose in such patients could be the identical on either methadone maintenance or buprenorphine maintenance. Naltrexone is a long-acting (24 to 48 hour length) opioid antagonist available in 50 mg tablets. It is effective in blocking the effects of opioids and can be utilized as a maintenance therapy, however its effectiveness has been limited by poor compliance. Compliance may be improved with behavioral therapy, however rates of retention in therapy nonetheless stay properly under what may be anticipated from agonist maintenance with methadone or buprenorpine. Rapid induction methods using buprenorphine, clonidine and clonazepam, have been described, however usually require 5 to 7 days to carry out. Special Considerations Methadone-maintained patients on medical-surgical items and pregnant patients benefit special remark. Drugs with combined antagonistagonist activity, such as pentazopcine and buprenorphine, might provoke opiate withdrawal and shoud be avoided. Women who turn into pregnant should be encouraged to contiue their methadone maintenance programme. The dose might must be reduced during the third trimester and neonatal signs due to abstinence should be deliberate for. Longitudinal studies present that infants exposed to methadone in utero develop usually and oldsters should be reassured. This part summarises the management of explicit psychiatric illnesses difficult by substance use and some related drug interactions. Drug Treatment for Specific Psychiatric Disorders There is controversy about the stage at which a temper dysfunction iunduced by substance abuse becomes a significant depressive episode. Most specialists will diagnose a second dysfunction in a affected person who presents with a depressive syndrome only after a 2 week period of sobriety. Clinical judgment is subsequently essential and, if a nonabstinent affected person has persistent melancholy, a trial of antidepressant therapy could also be carried out. Concurrent use of an antidepressant and a substance of abuse might enhance the chance of cardiotoxicity (arrhythmias), neurologic effects (seizures) or demise from intentional overdose. These dangers are biggest with the tricyclic antidepressants whereas the selective serononin reuptake inhibitors have a safer pharmacologic profile. Patients ought to always be discouraged from substance abuse however vital numbers of these taking antidepressants also use alcohol and different potential medicine of abuse in moderation with out harm. Antidepressants appear to have a low danger of abuse, although abuse of amitriptyline (for its sedative effects) and fluoxetine (for stimulant effects) has been reported. Substance abuse or dependence is a typical complication of schizophrenia and psychotic signs occurring during drug intoxication or withdrawal also complicate the prognosis of schizophrenia. An especially high degree of psychiatric sophistication and patience is necessary for this group of patients. Long-term studies (one 12 months) present that patients with schizophrenia and substance abuse want an lively therapy technique to interact them in therapy for psychosis, with an emphasis on compliance with antipsychotic treatment and the maladaptive effects of substance abuse. For most patients, the problem of substance abuse diminishes after a 12 months of compliance with treatment and therapy for dependancy. In this setting, using long-acting depot antipsychotic preparations is rational. Medication may also be combined with contingency contracting for patients with schizophrenia, making the unsupervised use of incapacity benefits contingent on unfavorable urine toxicology analysis.
Cheap tizanidine 2 mg amex
There are two types of feedback mechanisms: a negative feedback mechanism muscle relaxant reversal agents order tizanidine overnight delivery, which works to restore homeostasis by correcting a deficit throughout the system a positive feedback mechanism infantile spasms 8 months generic tizanidine 2mg on line, which happens when hormone secretion triggers further hormone secretion spasms hand purchase tizanidine mastercard. Accentuate the negative For negative feedback mechanisms to be effective muscle relaxant walmart order cheapest tizanidine and tizanidine, they have to sense a change in the body-corresponding to a excessive blood glucose stage-and attempt to return body capabilities to normal. In the case of a excessive blood glucose stage, the effector mechanism triggers elevated insulin production by the pancreas, returning the blood glucose stage to normal and restoring homeostasis. A positive feedback mechanism is liable for intensifying labor contractions during childbirth. The patient has subjective complaints, a particular medical historical past, and indicators, signs, and laboratory or radiologic findings characteristic of that illness. For example, a person might have coronary artery illness, diabetes, or bronchial asthma however not be unwell all the time as a result of his body has adapted to the illness. Diseases are dynamic and should manifest in numerous ways, depending on the patient and his setting. Intrinsic or extrinsic the reason for illness is intrinsic when the illness happens due to a malfunction or change throughout the body. Examples of extrinsic causes include infectious brokers, mechanical trauma, smoking, chemical exposure, dietary issues, drug use, temperature extremes, radiation exposure, and psychological stress. Unless recognized and efficiently treated, most ailments progress according to a typical sample of signs. Some ailments are selflimiting or resolve shortly with restricted or no intervention; others are persistent and by no means resolve. During exacerbation, the patient experiences an aggravation of signs or an increase in the severity of the illness. Telltale indicators Usually, a illness is uncovered due to an increase or lower in metabolism or cell division. Signs and signs might include hypofunction, corresponding to constipation; hyperfunction, corresponding to elevated mucus production; or elevated mechanical perform, corresponding to a seizure. How the cells reply to illness is determined by the causative agent and the affected cells, tissues, and organs. Disease levels Typically, ailments progress via these levels: � Exposure or damage. This second latent part happens in some ailments and is often followed by one other acute part. In this stage of rehabilitation, the patient progresses toward restoration after the termination of a illness. Stress and illness When a stressor corresponding to a life change happens, a person can reply in one of two ways: by adapting efficiently or by failing to adapt. Stressful levels Hans Selye, a pioneer in the study of stress and illness, described levels of adaptation to a tense event: alarm, resistance, and exhaustion or restoration. In the resistance stage, the body both adapts and achieves homeostasis or fails to adapt and enters the exhaustion stage, resulting in illness. Everything is underneath control the stress response is managed by actions happening in the nervous and endocrine systems. Mind�body connection Physiologic stressors might elicit a harmful response, leading to an identifiable illness or set of signs. Psychological stressors, such as the demise of a liked one, may trigger a maladaptive response. Stressful events can exacerbate some persistent ailments, corresponding to diabetes and multiple sclerosis. Types of cell damage Toxic damage-endogenous (metabolic errors, gross malformations, hypersensitivity reactions), exogenous (alcohol, lead, carbon monoxide, drugs) Infectious damage-viruses, fungi, protozoa, bacteria Physical damage-thermal (electrical, radiation), mechanical (trauma, surgery) Deficit damage-lack of primary requirement Maintaining homeostasis Medulla, pituitary gland, reticular formation are regulators. Two types of feedback mechanisms maintain homeostasis: � negative mechanism senses change and returns it to normal � positive mechanism exaggerates change. Influenced by genetic factors, unhealthy behaviors, personality kind, and notion of the illness. Manifests in numerous ways depending on Illness Occurs when a person is no longer in a state of "normal" health.
Consolida regalis (Delphinium). Tizanidine.
- What is Delphinium?
- Worm infestations, water retention, sleeplessness (insomnia), and lack of appetite.
- How does Delphinium work?
- Dosing considerations for Delphinium.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96435
Buy tizanidine online. Update on Esophageal Spasms.
Cheap tizanidine 2 mg online
See also Skin and delicate-tissue infections bacterial classification of spasms 2 purchase tizanidine 4mg amex, 449t proof-based mostly recommendations spasms movie generic tizanidine 4mg with visa, 450t�452t recommended oral drugs muscle relaxant at walgreens buy generic tizanidine 2mg online, 453t Solifenacin in prostate hyperplasia muscle relaxant benzo generic tizanidine 4 mg with visa, benign, 847t in urinary incontinence, 868t, 870, 870t Somatostatin in variceal hemorrhage, 247 Sorafenib as chemotherapeutic agents, 233t Sorbitol in constipation, 196�197, 198 Sotalol, 57 in antiarrhythmic drugs, 51t in arrhythmias, 50, 51t, 52t unwanted effects of, 54t Specific seizure disorders drugs of alternative for, 521t�524t Spermicide-implanted barrier methods, 261 Spermicides, 259t, 260t, 261 Spinal surgical procedure, surgical site infections in, 472t Spirometry in bronchial asthma, 822 Spironolactone in acne vulgaris, 139 in cirrhosis, 193t in coronary heart failure, eighty in hypertension, ninety four in myocardial infarction, secondary prevention after, 46 Spleen, abscess of, 400t Sponge, contraceptive, 260t, 261 Spontaneous bacterial peritonitis, 191�192 St. Oxford New York Auckland Cape Town Dar es Salaam Hong Kong Karachi Kuala Lumpur Madrid Melbourne Mexico City Nairobi New Delhi Shanghai Taipei Toronto With offices in Argentina Austria Brazil Chile Czech Republic France Greece Guatemala Hungary Italy Japan Poland Portugal Singapore South Korea Switzerland Thailand Turkey Ukraine Vietnam Copyright # 2007 by Oxford University Press, Inc. No part of this publication could also be reproduced, saved in a retrieval system, or transmitted, in any form or by any means, digital, mechanical, photocopying, recording, or in any other case, with out the prior permission of Oxford University Press. His pioneering studies into coma and its pathophysiology made the primary edition of this guide possible and have contributed to all the subsequent editions, together with this one. His insistence on excellence, though usually onerous to attain, has been an inspiration and a information for our careers. The authors also dedicate this guide to our wives, whose encouragement and assist make our work not solely possible but also nice. This page deliberately left blank Preface to the Fourth Edition Fred Plum got here to the University of Washington in 1952 to head up the Division of Neurology (within the Department of Medicine) that consisted of 1 individual, Fred. The University had no hospital but as an alternative used the county hospital (King County Hospital), now referred to as Harborview. The solely emergency room in the whole county was at that hospital, and thus it received all the comatose sufferers within the area. The solely noninvasive imaging obtainable was primitive ultrasound that might identify, typically, whether or not the pineal gland was within the midline. Thus, Fred and his residents (August Swanson, Jerome Posner, and Donald McNealy, in that order) looked for clinical methods to differentiate those lesions that required neurosurgical intervention from people who required medical treatment. In the Nineteen Fifties the one pH meter within the hospital was in our experimental laboratory and lots of the metabolic tests that we now consider routine had been time consuming and not obtainable in a timely trend. Yet the clinical strategy taught within the Diagnosis of Stupor and Coma remains the cornerstone of medical look after comatose sufferers in just about each hospital, and the necessity for a modern updating of the textual content has been clear for some time. At the identical time, there was substantial progress in concept on the neural basis of consciousness, and the senior author wished to incorporate as a lot of that new material as possible into the new edition. A second impediment to the early completion of a fourth edition was the retirement of the senior author, who also developed some problem with expressive language. It grew to become obvious that the senior author was not going to be able to full the new edition with the eloquence for which he had been identified. Fred participated within the initial drafts of this edition, but not totally within the ultimate product. Thus, the errors and wrongheaded opinions you would possibly find in this edition are ours and not his. We as his college students feel privileged to be able to proceed and update his classic work. One of our most essential goals was to retain the clear and authoritative voice of the senior author within the current revision. Even although a lot of the textual content has been rewritten, we worked from the original organizational and conceptual context of the third edition. Because the clinical examination remains largely unchanged, we may use a number of the case reviews and lots of the figures describing the clinical examination from earlier editions. Fred was present at every of the critical editorial conferences, and he continued to contribute to the general construction and scientific and clinical content of the guide. Most essential, he instilled his concepts and views into every of the other authors, whom he taught and mentored over many years. However, every of the chapters was handed back and forth and revised and edited by every of the authors, in order that the duty for the content of the fourth edition remains joint and a number of other. The examination of the comatose patient remains the cornerstone to clinical judgment. It is way sooner and extra correct than any imaging study, and correct clinical evaluation is necessary to determine what steps are required for additional analysis, to determine the tempo of the workup, and most essential, to identify those sufferers in critical situation who want emergency intervention. Coma remains a classic drawback in neurology, during which intervention inside minutes can usually make the difference between life and demise for the patient.
Buy tizanidine on line amex
Mechanical ventilation was instituted and blood strain was supported with pressors muscle relaxant gel india cost of tizanidine. On examination she had spontaneous eye actions within the vertical course only and her eyelids fluttered open and closed muscle relaxant at walgreens tizanidine 4 mg without a prescription. There was complete flaccid paralysis of the hypoglossal spasms constipation order tizanidine online from canada, vagal muscle relaxant cyclobenzaprine high buy tizanidine in united states online, and accent nerves, as well as all spinal motor operate. The patient responded to commands to open and shut her eyes and realized to talk in this means. She lived one other 12 weeks in this setting, with out regaining operate, and rarely was noticed to sleep. However, the injection of ethanol had apparently entered the C2 root sleeve and glued the lower brainstem up through the facial and abducens nuclei with out clouding the state of consciousness of the patient. Comment: Both of these cases demonstrated the preservation of consciousness in patients with a locked-in state because of destruction of motor pathways under the crucial level of the rostral pons. Chapter 2 will explore the methods during which the neurologic examination of a comatose patient can be utilized to differentiate these totally different causes of loss of consciousness. Four days before she died, she developed ocular bobbing when commanded to look laterally, however although she persistently responded to commands by shifting her eyes, it was tough to know whether or not her responses had been applicable. The mind at autopsy contained a moderate quantity of darkish, old blood overlying the best lateral medulla adjoining to the fourth ventricle. On section, the vascular malformation was seen to originate within the central medulla and to lengthen rostrally to approximately 2 mm above the obex. From this point, a large hemorrhage prolonged ahead to destroy the central medulla all the way to the pontine junctionure 1�9B). Microscopic study demonstrated that, at its most cranial finish, the hemorrhage destroyed the caudal part of the best vestibular nuclei and a lot of the adjoining lower pontine tegmentum on the best. Caudal to this, the hemorrhage widened and destroyed the complete dorsal center of the medulla from approximately the plane of the nucleus of the glossopharyngeal nerve right down to just under the plane of the nucleus ambiguus. From this latter point caudally, the hemorrhage was more restricted to the reticular formation of the medulla. The margins of this lesion contained an organizing clot with phagocytosis and reticulum formation indicating a course of at least 2 weeks old. The center of the hemorrhage contained a degenerating clot estimated to be at least seventy two hours old; at a number of locations along the lateral margin of the lesion had been small contemporary hemorrhages estimated to have occurred within a number of hours of demise. It was thought of unlikely that the lesion had changed considerably in measurement or extent of destruction within the few days before demise. Neuropsychiatric findings in anti-Ma2-optimistic paraneoplastic limbic encephalitis. She had rheumatoid arthritis with subluxa- Pathophysiology of Signs and Symptoms of Coma encephalopathy. Treatment of cobalamin deficiency in dementia, evaluated clinically and with cerebral blood flow measurements. Hallucinations and delusions following a proper temporoparietooccipital infarction. The vegetative and minimally acutely aware states: consensus-based criteria for establishing analysis and prognosis. Review by a working group convened by the Royal College of Physicians and endorsed by the Conference of Medical Royal Colleges and their Faculties within the United Kingdom. The effects of posterior hypothalamic lesions on behavioral and electrographic manifestations of sleep and waking in cat. Forebrain inhibitory mechanisms: sleep patterns induced by basal forebrain stimulation within the behaving cat. Nucleus basalis and thalamic management of neocortical activity within the freely shifting rat. Ascending conduction in reticular activating system, with particular reference to the diencephalon. The origins of cholinergic and different subcortical afferents to the thalamus within the rat. Adenosinergic modulation of basal forebrain and preoptic/ anterior hypothalamic neuronal activity within the management of behavioral state. Sleepwaking discharge patterns of ventrolateral preoptic/ anterior hypothalamic neurons in rats.
Cheap tizanidine 2mg without prescription
However muscle relaxant methocarbamol tizanidine 4mg lowest price, different mothers become anxious muscle relaxant non-prescription generic 4mg tizanidine mastercard, fatigued muscle relaxant uses purchase 2mg tizanidine amex, or depressed muscle spasms 2 weeks tizanidine 4mg otc, and consequently they inadvertently intensify the feeding difficulties of their infants. This feeding dysfunction has been referred to within the early literature as maternal deprivation, deprivation dwarfism and psychosocial deprivation. The progress failure and developmental delay of those infants have been considered a consequence of a continuum of neglect and/or maltreatment of the child resulting in insecure attachment to the caregiver. Diagnosis Young infants who present with feeding difficulties and progress failure relationship to the postnatal interval need to be considered for the prognosis of a feeding dysfunction of state regulation. However, there appears to be an increased prevalence of instances within the lower socioeconomic classes, as noted by Chatoor and colleagues (1997). Etiology Much has been written about mothers whose infants fail to thrive and appear to have a dysfunction of reciprocity. They are incessantly described as affected by character dysfunction, affective illness, alcohol abuse and drug abuse. Family problems and distressed marital relationships have been reported in numerous noncontrolled and managed research of failure to thrive. In addition, socially adverse living circumstances, poverty and unemployment are reported to be more prevalent in these families of infants with failure to thrive. Mothers of infants with failure to thrive are more likely to be classified as insecurely connected to their very own parents, as measured by the Adult Attachment Interview (Main and Goldwyn, 1991). The progress failure of those infants with poor caregiver� toddler reciprocity appears to be a critical manifestation of a failed relationship between a mother and her toddler in the course of the first year of life, when the foundation for mutual engagement and attachment is usually laid. Course and Natural History During the primary few months of life, the foundation for the regulation of feeding, sleep and emotions is laid. Infants with feeding problems during these early months usually set off nervousness of their mothers and tend to have difficulties in self-regulation in the course of the transition to self-feeding within the second year of life. Treatment Treatment can be directed towards the toddler, towards the mother, and towards the mother�toddler interplay. This will allow an anxious mother to chill out as a result of her toddler is receiving sufficient vitamin to develop. Subsequently, a more relaxed mother can tune into her toddler more readily and break the cycle of dyadic escalation of rigidity during feedings. On the opposite hand, the intervention might need to be directed primarily towards the mother to treat her nervousness, fatigue, or despair to allow her to be simpler in coping with her toddler. In addition, most mothers can be helped by helping them in downside solving in tips on how to facilitate a feeding environment that gives the optimal amount of stimulation for his or her vulnerable infants. Because of their severe failure to thrive, these infants incessantly require hospitalization. A psychological standing examination of the mother must be carried out to rule out severe psychiatric illness, notably whether she suffers from despair or is abusing alcohol or medicine. Consequently, the remark of Feeding Disorder of Poor Care Giver�Infant Reciprocity Diagnostic Criteria A. Infants with feeding issues of poor mother�toddler reciprocity characteristically feed poorly, keep away from eye contact and are weak within the first few days of hospitalization. When picked up, they might scissor their legs and hold up their arms in a give up posture to steadiness their heads, which seem too heavy for his or her little weak bodies. However, these infants appear to blossom underneath the tender care of a primary care nurse who engages with them during feeding and plays with them. They become increasingly responsive, start to smile, feed hungrily and achieve weight. In basic, nonorganic failure to thrive during infancy has been related to later cognitive and behavioral problems. Hufton and Oates (1977) reported that of 21 youngsters who had been identified with nonorganic failure to thrive during infancy, on the age of 6 years, half of the kids had irregular personalities and two-thirds had a delayed studying age. Nurturance of the mother is the primary critical step within the therapy to facilitate her potential to nurture her toddler. The hospitalization of the toddler supplies a critical time to assess whether the toddler needs to be placed in various care.
Order tizanidine paypal
The routine must be based mostly on in vitro sensitivity tests Intraabdominal Infections Peritoneal dialysis Initial empiric regimens must be energetic towards both Gram-constructive (together with S spasms cerebral palsy purchase generic tizanidine on-line. Ceftriaxone muscle relaxant 8667 purchase tizanidine now, cefotaxime spasms 1983 wikipedia buy tizanidine 4mg mastercard, or antianaerobic cephalosporinsa Other Third- or fourth-generation cephalosporin with 1 muscle relaxant usage buy discount tizanidine on-line. Ciprofloxacinb or levofloxacinb every with metronidazole or moxifloxacinb alone metronidazole, piperacillin�tazobactam or 2. Aztreonam with vancomycin and metronidazole ticarcillin�clavulanate, carbapenem 3. Antianaerobic cephalosporinsa Abscess General Third- or fourth-generation cephalosporin with 1. Imipenem�cilastatin, meropenem, doripenem, or ertapenem metronidazole, piperacillin�tazobactam, or ticarcil- 2. Ciprofloxacin b or levofloxacin b every with metronidazole or moxifloxacin lin�clavulanate alone Liver As above Use metronidazole if amoebic liver abscess is suspected Spleen Ceftriaxone or cefotaxime Moxifloxacinb or levofloxacinb Other Intraabdominal Infections Appendicitis Same management as for neighborhood-acquired difficult intraabdominal infections as listed in Table 92-639 Community-acquired Ceftriaxone or cefotaxime Severe an infection, piperacillin/tazobactam, antipseuodomonal acute cholecystitis carbapenem, aztreonam with metronidazole Cholangitis Ceftriaxone or cefotaxime every with or without Vancomycin with aztreonam with or without metronidazole metronidazole Acute contamination from Antianaerobic cephalosporinsa or metronidazole 1. Piperacillin/tazobactam or a carbapenem stomach trauma with both ceftriaxone or cefotaxime 2. Ciprofloxacinb or levofloxacinb every with metronidazole or moxifloxacin alone Cefoxitin or ceftizoxime; these agents must be prevented empirically unless local antibiograms present >80% to 90% susceptibility of E. Use of quinolones could also be related to treatment failure as a result of increasing resistance of enteric pathogens together with E. These agents embody meropenem, imipenem�cilastatin, doripenem, piperacillin�tazobactam, or ceftazidime or cefepime together with metronidazole. Aregimencanbeconsidered unsuccessful if a significant antagonistic drug reaction happens, if reoperation is necessary,orifpatientimprovementisdelayedbeyond1or2weeks. The widespread chilly viruses together with rhinovirus and coronavirus and lower respiratory tract pathogens together with influenza virus, adenovirus, and respiratory syncytial virus, account for the majority of circumstances. Recurrentacuterespiratory infectionsmaybe related to elevated airway hyperreactivity and probably the pathogenesis of chronicobstructivelungdisease. Clinical Presentation �Acute bronchitis normally begins as an upper respiratory an infection. Treatment �Goals of Therapy:Thegoalistoprovidecomforttothepatientand,intheunusually �The treatment of acute bronchitis is symptomatic and supportive in nature. In otherwise wholesome patients, no meaningful benefitshavebeendescribedwiththeuseoforaloraerosolized2-receptoragonists and/ororaloraerosolizedcorticosteroids. Expectoration of the most important quantity of sputum normally happens upon arising within the morning, although many patientsexpectoratesputumthroughouttheday. The most common bacterial isolates (expressed in percentagesoftotalcultures)identifiedfromsputumcultureinpatientsexperiencing anacuteexacerbationofchronicbronchitisaregiveninTable forty three�1. Clubbing of digits (advanced illness) Obesity Chest radiograph Increase within the anteroposterior diameter of the thoracic cage (noticed as a barrel chest) Depressed diaphragm with limited mobility Laboratory tests Erythrocytosis (advanced illness) Pulmonary function tests Decreased very important capability Prolonged expiratory circulate �Withtheexceptionofpulmonaryfindings,thephysicalexaminationofpatientswith mildtomoderatechronicbronchitisisusuallyunremarkable(Table forty three�2). Agentsshouldbeselectedthatareeffectiveagainstlikely pathogens,havethelowest riskof drug interactions, andcan beadministeredin a mannerthatpromotescompliance(seeFig. Clinical Presentation �The most common medical indicators of bronchiolitis are found in Table forty three�4. A pro- drome suggesting an upper respiratory tract an infection, normally lasting from 2 to eight days,precedestheonsetofclinicalsymptoms. Asaresultoflimitedoralintakedue to coughing mixed with fever, vomiting, and diarrhea, infants are frequently dehydrated. Otherwise wholesome infants can be handled for fever, supplied beneficiant amountsoforalfluids,andobservedclosely. Use of the drug requires special gear (small-particle aerosol generator)andspecificallytrainedpersonnelforadministrationviaoxygenhood ormisttent. Obtundation, hallucinations, grand mal seizures, and focal neurologic findings have also been associated withthisillness. Anaerobic Pneumonia �Thecourseofanaerobicpneumoniaistypicallyindolentwithcough,low-gradefever, and weight loss, although an acute presentation may occur. Systemic symptoms usually clear in 1 to 2weeks, whereasrespiratorysymptomsmaypersistupto4weeks. Viral Pneumonia �The medical pictures produced by respiratory viruses are sufficiently variable and overlaptosuchadegreethatanetiologicdiagnosiscannotconfidentlybemadeon clinicalgroundsalone.